Surgery
The surgery is done by a direct minimally invasive approach (a small skin incision is made, muscles are not cut) using surgical magnifying loupes and under endoscopic control.
Robot-assisted surgery is possible only in case of one nodule, less than 2 cm in size, without suspicion for metastasis in neck lymph nodes. This surgery is performed by transaxillary approach – the surgery lasts more time.
Neuromonitoring system is systematically used during surgery to control the position of the recurrent nerve and prevent its injury.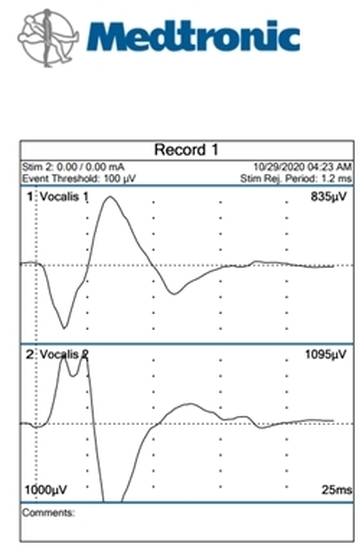
1. A nodule (several nodules) suspicious for cancer.
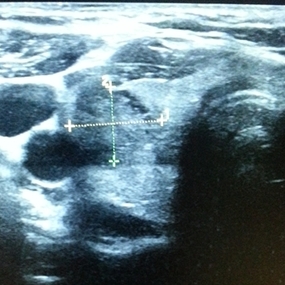
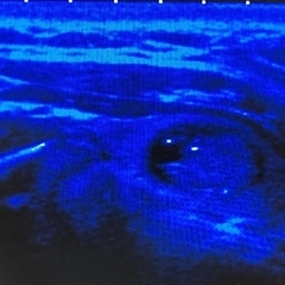
4 specialists work in a team- an endocrinologist, an ultrasound specialist, a histologist and a surgeon. Dr. Jean-Rene Milliet is present during thyroid ultrasound to elaborate a common opinion about EU-TIRADS classification with ultrasound specialist.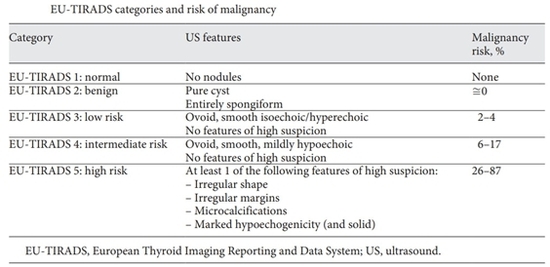
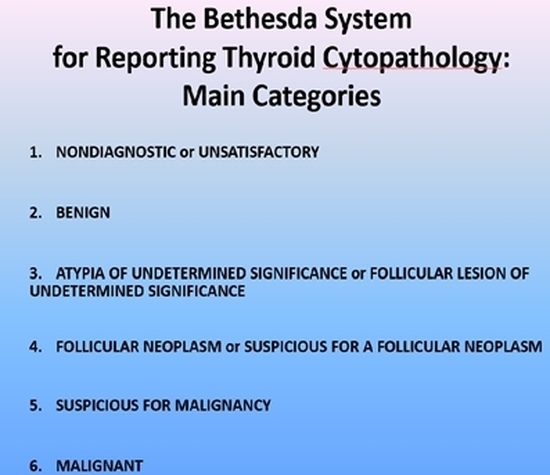
Fine needle aspiration biopsy of the thyroid nodules is made by an experienced ultrasound specialist in the presence of cytologist, if it`s possible. The cytologist will give a BETHESDA classification in the conclusion. Depending on the cytology results other specific examination can be performed, such as immunocytochemistry and a second opinion review of thyroid FNA.
The patient can be given a choice:
- perform hemithyroidectomy and wait for the final histology conclusion (follicular cancer, central papillary cancer T1 a -N0).
- Total thyroidectomy, sometimes with intraoperative histology and neck lymph nodules removal.
2. Hyperthyroidism:
endocrinologist role is fundamental in this case. It`s him (her) who makes a decision about thyroid surgery necessity. The type of hyperthyroidism will be specified on scintigraphy. Thyroid ultrasound will show the anatomy and location of a toxic thyroid nodule and presence of other nodules. A patient with a toxic thyroid nodule will be recommended hemithyroidectomy, while a patient with Basedow`s disease ( Graves` disease) will be indicated total thyroidectomy.
3. A big nodule :
isolated nodule or several nodules. The thyroid can grow down into the chest. Before surgery it`s necessary to do a CT of the neck and the chest with contrast.
